

"I grew up in Caracas, Venezuela, in a time when the signs of economic collapse were already starting to show.
I practiced medicine at the three main hospitals in the capital: Hospital Miguel Perez Carreno Hospital Universitario de Caracas Hospital Domingo Luciani."
In 2017 I went to live and practice medicine deep inside the Amazon jungle.
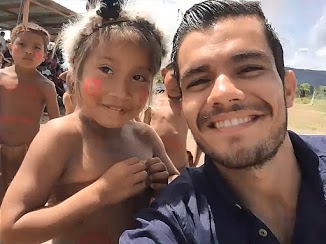
Away from civilization, I had to make do with what I had on hand to perform a wide range of medical procedures for accidents, diseases and delivering babies
I made use of traditional methods when supplies were scarce, like cleaning wounds with antiseptics and honey as a Bacteriostatic (substance that stop bacterial reproduction but doesn't kill them), until more supplies arrived.

I can truly say that there is a BIG difference between the kind of medicine a doctor has to practice there and what is being done in hospitals using the latest technology, CT scans, blood tests, electro-microscopes, X-rays, dialysis machines, ventilators, etc. When we ran out of bandages we had to learn what kind of leaves are good for replacing them. To be a doctor in a remote area you need a different type of knowledge than the one they teach you in medical school. In my opinion it is similar to the kind you need to help yourself out or someone else during a crisis, when medical assistance becomes unpredictable and life-saving supplies run low.

What few people realize is that when that happens many common conditions, easily treatable today, become life threatening.
For example, an Asthma attack, which is manageable at home with the right medicine, turned extremely dangerous after supplies ran out in the Amazon. We barely saved a 4 year old cyanotic boy (blue discoloration of the skin when lack of oxygen) suffering an Asthma attack.
We diagnosed over 50 people with Malaria and provided the most basic treatment that anyone can apply to every patient saving them from a deadly disease.

Back in Caracas, I was also part of the Green Cross, a group of front-line paramedics that helped both injured protesters and law enforcement alike; anyone who needed help during the protests was aided. On the green cross project, we attended multiple emergencies and one of the most common things that we dealt with was pepper gas intoxication. We treated them with asthma inhalers and "Malox" a well-known antiacid mixed with water that we sprayed in peoples face for reducing the face burning and itching (it alleviated the pepper gas effect).

During my surgery rotations, we lacked some of the essential supplies needed to attend thoracic penetrating traumas (knife and gun fire wounds). After extracting the bullet or solving the internal problem the patient needs a "pleur-evac" (drainage system for the thoracic cavity) for draining all inflammatory or rests of blood on the thorax avoiding respiratory problems. In our cases we build them with a 5lt water bottle, some water and artisanal tubes saving most of these patient lives and maintaining an adequate live support.

I am currently a Postdoctoral Research Associate for the department of Surgical Oncology at UT Southwestern Medical Center in Dallas, Texas. I'm administering the Robotic curriculum of the surgery residence, training residents on their robotic skills.
The breakthroughs that we are pioneering here will make a big difference for patients with oncological pathologies. We are able now to make more precise incisions and save more patients than through conventional methods. But, in the next crisis, it is the old methods that we will need to have by our side when the grid goes down and supply chains break down.
© 2021 All Rights Reserved